
In this blog we will present you a practical case of layering in a class IV composite restoration made with G-aenial A'CHORDand you will learn about the great characteristics and ease of use of this advanced GC product with which you can obtain truly biomimetic results, aesthetic and durable. Are you ready? Let's start!
In the layering of direct composite restorations, the combination of the optical properties of the different layers of the composite is used in order to simulate the color, characteristics and translucency of natural teeth.
Significant improvements in composite technology have made it possible to simplify this procedure, which was not considered complex until very long ago. However, today there are difficulties in imitating the remaining dentin structure when restoring anterior teeth due to the great variety of colors, intensity and levels of translucency of many current composite systems.
The G-aenial A'CHORD composite is the evolution of the G-aenial system, which has been successfully used in dental clinics for the last 10 years. In contrast to its predecessor, G-aenial A'CHORD is an improvement in the following features:
- It is aesthetic and harmonious under any light, it has natural fluorescence.
- It is very easy to sculpt with conventional composite modeling instruments or restoration brushes, thanks to its optimal handling properties.
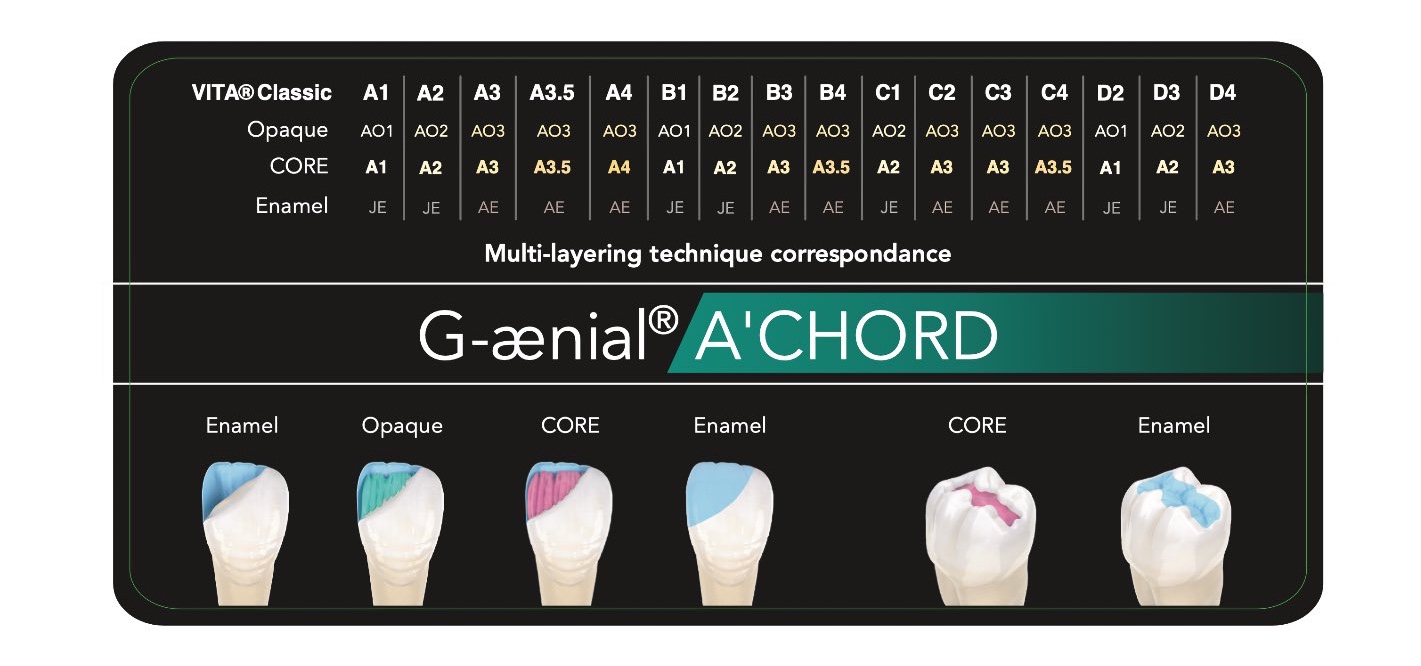
- It allows a high polish and shine in very few steps, due to its Full Coverage (FSC) silane-type coating technology that covers nanofillers with a silane coupling agent.
- It incorporates opaque colors of additional enamel, allowing infinite possibilities of opacity and values.
- 5 CORE shades cover 16 VITA shades, which is a great simplification.
Practical case of stratification with G-aenial A`CHORD of GC
This case study demonstrates the use of GC Europe's G-aenial A'CHORD direct composite system in a complex class IV restoration in a 22-year-old female patient.
The patient comes to the clinic due to the disagreement with an existing restoration of an upper left central incisor (Piece 21 FDI) and requests the replacement of the restoration with one that is conservative, imperceptible and that allows her to have a normal social life. The patient indicates that her previous dentist has performed this class IV restoration four times but the result has never been satisfactory for her.
Clinical examination reveals a high smile line with symmetrical and esthetic gingival architecture . The existing composite restoration on tooth 21 was clinically acceptable, however it did not integrate with the tooth color or with the other teeth. Discoloration and slight protrusion could be seen on the disto-labial aspect and this indicated the possibility of marginal leaks.
In the preoperative shade evaluation it could be seen that tooth 21 was slightly more chromatic than the adjacent upper right central incisor (tooth 11). The maxillary left central incisor (item 21) also had a slight labial shift in its alignment compared to the adjacent tooth 11.
Regarding the medical history of the patient, there was nothing relevant.
In the radiographic and periodontal examination it was observed that tooth 21 did not present pathologies or problems that required attention before performing the restoration and the response to the thermally tested pulp vitality test was normal.
The patient was presented with three treatment options, carefully identifying the advantages and disadvantages of each:
- A ceramic veneer with tissue reduction on tooth 21.
- A full composite veneer of tooth 21. Bearing in mind that due to the slight labial lateral displacement of tooth 21, very little labial reduction would be needed to allow space to mask the chromatic dentin.
- A complex and conservative class IV restoration of tooth 21 had to be additionally completed to minimize any preparation and reduction of tooth structure.
The patient's choice was the conservative approach to treatment that included an added protocol (option 3). She stated that she would be satisfied with a harmonious composite restoration of tooth 21 and that the chromatic part did not concern her esthetically.
The final plan from the clinical point of view was to restore tooth 21 with a direct composite restoration , with a conservative, long-lasting approach and a biomimetic final result, an optimal aesthetic and morphological integration with the natural teeth.
Step by step class IV restoration with G-aenial A`CHORD from GC
Before starting the restoration process, clinical photographs and color selection were made. Diagnostic impressions were also taken to subsequently manufacture the silicone or matrix palatal splint to facilitate the three-dimensional plane of the stratification of the composite increments.

Figure 1: Preoperative view without retraction, showing the non-aesthetic and failed direct composite restoration in tooth 21 (upper left central incisor.
Figure 2: Preoperative view with retraction a) with regular light flashes b) with polarized filter.

Figure 3: Isolation of the work field was done by using a rubber dam. Existing restoration and caries were removed and a 2mm bevel was prepared at the labial margin of the preparation to improve the esthetic and functional integration of the composite restoration with the remaining natural tooth structure.
Figure 4: The bevel was prepared with a Komet conical diamond bur. All transition angles of the cavity were rounded off with an oval or egg-shaped polishing bur. The burs are part of the Dr. Anthony Mak Custom C&B Selection kit from Komet Dental .
Figure 5: The palatal key was cut and tested to check the fit of the silicone matrix and to ensure that the dam and clamps do not interfere with its seating.

Figure 6: The cavity was cleaned prior to the air bonding procedure with Velopex AquaCare 29 micron aluminum oxide powder and Teflon (PTFE) tape was used to prevent accidental bonding to adjacent teeth.
Figure 7: The adhesive procedure was started with selective etching of the cavity with Ultradent 37% phosphoric acid Ultra-Etch. Subsequently, the etching gel was washed off and the adhesive process was completed with the application of a universal bonding agent: G-Premio BOND from GC Europe . The universal adhesive was then dried for 5 seconds with maximum pressure air and light-cured for 10 seconds according to the manufacturer's instructions.
Figure 8: Continuing with the adhesive protocol, a thin layer of semi-translucent G-aenial A'CHORD enamel shade JE (GC Europe) was used to create the palatal surface.

Figure 9: Next, the interproximal wall was made using the same semi-translucent G-aenial enamel color A'CHORD color JE (GC Europe). The interproximal wall was shaped using a plastic strip and the extraction technique to help create an anatomical contour.
Figure 10: The dentin layer was then completed by adding an opaque shade, G-aenial A'CHORD shade AO2 (GC Europe). This increment was designed to simulate extensions of the natural morphology of the dentin core and was extended until it was subtly shorter than the prepared bevel. The dentin or opaque shade provides the optimal opacity for the final restoration.
Figure 11: A G-aenial A'CHORD color A2 (GC Europe) body chromatic shade was applied and extended beyond the bevel to disguise the transition line. The mamelons of the incisal third were also sculpted and formed in this increase of composite resin.
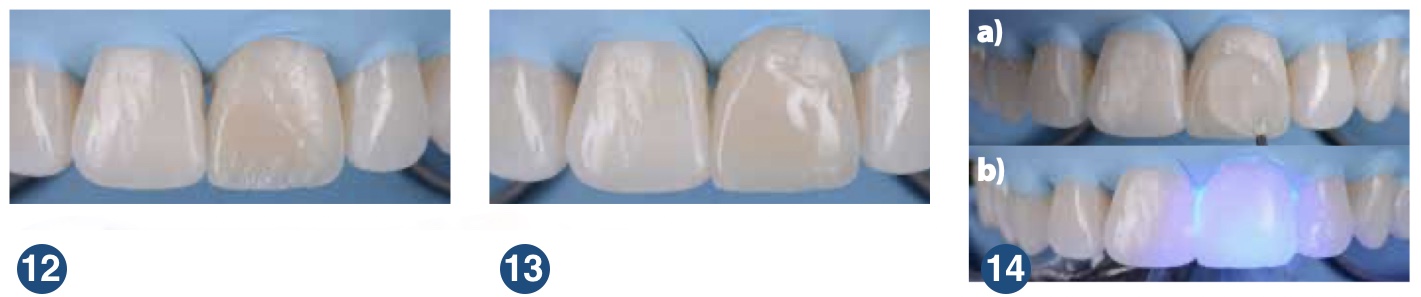
Figure 12: Comparisons with polarized diagnostic photographs taken prior to the start of the restoration provided guidance for the incorporation of these internal features.
Figure 13: A final translucent shade G-aenial A'CHORD shade JE (GC Europe) was then layered to produce the full contour anatomy for a natural optical blending effect.
Figure 14 a and b: Subsequently, glycerin gel was applied to the buccal surface of the restoration and light cured to enhance the polymerization of the direct layered composite restoration due to the absence of an oxygen inhibition layer.

Figure 15: The restoration was polished and finished to incorporate the primary, secondary, and tertiary anatomy in order to obtain a realistic restoration that mimics the adjacent right central incisor (item 11).
Figure 16: Soflex discs from 3M-ESPE and Komet diamond polishing burs were used for polishing and finishing, followed by a stepped sequence of Astropol silicone polishers and finishers from Ivoclar-Vivadent. The restoration was then completed with a GC Europe DiaPolisher Paste on a Cosmedent Flexi-Buff felt to reproduce the natural gloss of the enamel.

Figure 17: Immediately after restoration (no shrinkage). The finished and polished G-aenial A'CHORD restoration has a morphological and optical aesthetic integration of the complete restoration in the patient's natural dentition.
Figure 18: Immediately after the operation (with retraction): seen in a) Normal flashes of light; b) Polarized filters.


Figure 19 and 20: Revision after two weeks demonstrates complete optical and functional restoration of the G-aenial A'CHORD in tooth 21.
Conclusion
Advances in monochromatic universal composite systems for anterior restorations continue to improve, but layering techniques for the application of a truly esthetic direct anterior composite restoration will always be needed in the dental practice. This is due to the intrinsic anatomy of the natural tooth, where simulation of the optical and morphological properties cannot be achieved with a single mass of restorative material. GC Europe's A'CHORD G-aenial Composite System offers a simple approach to the staining/layering process, while providing an end result that is truly biomimetic, esthetic and durable .
If this clinical case has been useful for your clinical practice, don't be left wanting to test the surprising properties of GC's G-aenial A'CHORD composite and request your free sample today (only in Spain).
I want a sample of G-aenial A'CHORD!
And if you have already decided and want to achieve the best and most aesthetic results with G-aenial A'CHORD from GC Europe , remember that this product is available at Dentaltix in its practical syringe and Unitip presentations.


If you want to be aware of all the news in the dental sector and the best clinical cases, remember to follow us on our social networks and if you have any questions, contact us so that we can help you. See you soon!





